
Substance Use Disorders
-
A Substance Use Disorder (SUD) or addiction is a chronic relapsing disease of the brain effecting the reward, motivation, and memory circuitry.
-
SUD is not a moral failing. No one woke up one day and said "I'm going to become a heroin addict", or "I've decided to lose my job, friends, and family because of my drinking". SUD is not a life choice.
-
By definition, it's the continued use of the drug, inability to stop, despite attempts to stop or cut down, loss of family, friends, job or housing, or negative physical effects such as liver damage, GI bleeds, abscesses, endocarditis or overdose.
-
Reward center of brain exists for survival. Reward center is strongly affected by food and sex. Also activated whenever a sense of "well being" is felt e.g. finding a great sale item on-line or seeing your newborn baby for the first time! Triggers surges of endogenous opioids and dopamine causing "pleasure".
-
How many of us have tried to lose weight but can't? Food gives us pleasure despite knowing it can be very unhealthy and increases risk for chronic disease.
-
Drugs/alcohol cause exponentially higher surges of these endogenous opioids and dopamine. BRAIN WANTS TO REPEAT THIS OVER AND OVER!
-
Addiction behaviors (e.g. drug use) stimulate the reward center despite negative consequences.

Chronic Medical Conditions such as DM, HTN, or COPD
Inheritable with genetic and environmental components.
Chronic medical diseases result from damage to heart, lungs, kidneys, etc.
Cardiomyopathy/CHF due to CAD, infection, drugs etc can result in decreased ejection fraction. Imaging studies can how poor perfusion or poor function. Would you tell the patient "Make your heart pump better"
Relapse rates defined as ongoing symptoms of active disease requiring medical intervention to modify treatment or lifestyle. Relapse rates: Asthma 50-70%, HTN 50-70%, Diabetes 40-60%
Treatment involves combination of lifestyle changes, social support plus medication e.g. inhalers, ACE inhibitors, metformin
Chronic disease are considered to be lifelong with no cure. Medications/support services are used to keep diseases in remission, under control. Medication treatment is considered to be needed for life. You'd never tell a patient with HTN that he'll be in treatment for only 4 weeks and then off medication.
We use words like "patient, victim, suffer, survivor, fighter, endure, afflicted" We don't blame the patient. It's a disease that happened TO the patient. Our attitude is it's not the patient's fault. We'd never call a patient with diabetes "A sugar abuser" or say to a patient "Your blood is dirty with cholesterol".
Acute events presenting to the ED like acute CHF are treated quickly and with respect. Imagine treating an acute MI with blaming the patient, withholding care until patient agrees to go to weight loss classes or handing the patient a list of cath labs for them to find their own cardiologist or kicking the patient out of the hospital if they had recurrent chest pain.
We use laboratory and imaging studies to monitor chronic diseases and help with treatment decisions. We follow glucoses for diabetes, renal function for transplant patients, and O2 sats in patients with COPD. Helps avoid negative consequences.
We make every attempt to treat patients with compassion and respect.
We'd never arrest someone for not managing their diabetes, continuing to smoke or not losing weight. All of these contribute to ongoing chronic diseases which contribute to health care costs. We don't blame the patient. We don't arrest our way to good healthcare.
Staying in long term treatment is considered a success.
Substance Use Disorders
Inheritable with genetic and environmental components.
Substance Use Disorders result from injury to the brain.
Often frontal lobe injury result from chronic drug or alcohol use. Imaging studies changes that may be permanent. Frontal lobe controls decision making, weighing consequences or risk/benefits, delayed gratification. Reward circuitry of the brain is on overdrive. Telling someone "Just make better decisions" doesn't work.
Relapse rates defined as ongoing symptoms of active disease requiring medical intervention to modify treatment or lifestyle. Relapse rates: SUD 40-60%
Treatment involves combination of lifestyle changes, social support plus medication e.g. buprenorphine, naltrexone.
SUDs are often treated like an acute diseases that can be "cured" in just a few weeks of counseling or medication. MRI studies show it can take several years for brain injuries from SUD to recover.
Stigma surrounds SUDs. We use words like "abuse, abusers, misuse, clean, dirty, addict, junkie". We blame the patient. It's the patient's fault. "Abuser" is used for domestic violence, sexual assault and child abuse. These are violent acts and the word should not be connected with a chronic disease. Words matter and can immediately change our interactions with patients. Person first language!
Patients suffering from SUD are often told they are to blame for their disease, if only they made better choices; they have to agree to go to "treatment" or "counseling" in order to get acute care in a hospital, they are handed telephone numbers and told "find your own treatment center" and if they are found using drugs in the hospital, they are kicked out.
We use laboratory tests such as urine tox screens to punish the patient. Positive drug screens are considered failures by the patient. Instead should be used to have a conversation. To help avoid long term consequences such as liver disease or endocarditis or high risk situations like overdose.
We often feel we need to "punish" the patient. Make care difficult or unpleasant.
Drug use is treated as a crime instead of a chronic medical condition. We arrest patients who use drugs. Hospitals need to be safe havens for patients. They should not worry they will be arrested for use or possession.
Needing longterm treatment is considered a failure and should, instead, be considered standard and necessary for disease management.
Stigma Language
Stigma toward patients with SUDs is manifested in many ways including the words we choose. Research shows patients are treated differently when words such as "addict" or "drug abuser" are used when discussing patient care.
Instead of...
Addict
Alcoholic
Drug problem, drug habit
Drug abuse
Drug abuser
Clean / Abstinent
Dirty
A clean drug screen
A dirty drug screen
Former / reformed addict/alcoholic
Opioid replacement, methadone maintenance
Detox
Consider...
Person with substance use disorder or SUD
Person with alcohol use disorder or AUD
Substance use disorder
Drug misuse, harmful use
Person with substance use disorder
Abstinent, not actively using
Actively using
Testing negative for substance use
Testing positive for substance use
Person in recovery, person in long-term recovery
Medications for addiction treatment
Medically-assisted withdrawal

DSM 5 Criteria
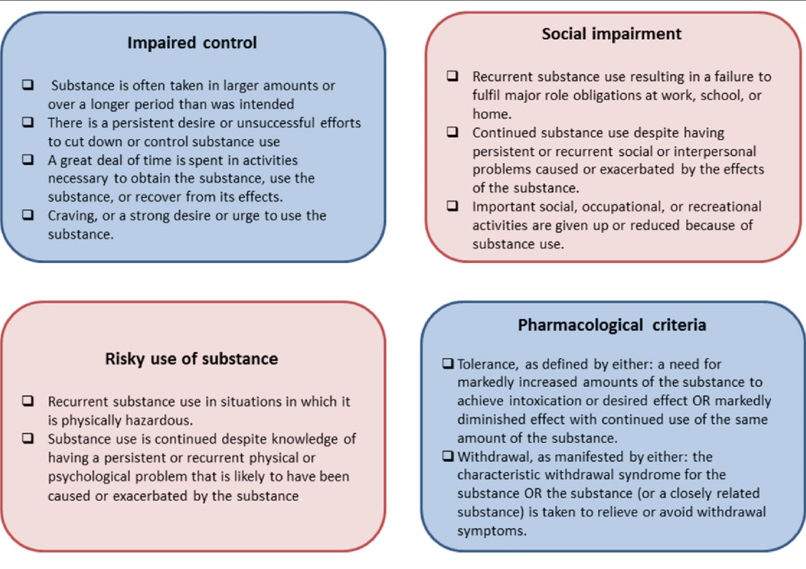
SEVERITY - Mild: 2-3, Moderate: 4-5, Severe: 6+
"Morning" - In the morning, do you ever use/drink in order to not feel sick/not shake/calm your nerves? (Withdrawal)
"More" - Do you need to use more/drink more to get the same high/feeling as when you first started using/drinking?" (Tolerance)
"Miss" - Do you ever miss family events, work, doctor's appointments because of your use/drinking? (Social Impairment)
"Spend" - Do you spend a lot of time looking for drugs/alcohol, using drugs/alcohol, or recovering from drug use/alcohol? (Impaired Control)
"Sick" - Do you realize your medical problems (e.g. cirrhosis, overdose, abscess, endocarditis) is the result of your drug/alcohol use, but you still use/drink? (Risky Behavior)
"Stop" - Have you ever tried to stop using/drinking but couldn't? (Impaired Control)

Why should EDs care?
-
We see these patients every day in the Emergency Department and for some patients, we see them a lot!
-
Patients with substance use disorders often do not go to primary care. Their only interaction with the healthcare system is the ED.
-
Patients may be willing to get treatment for their SUD when they've had an MVA due to drinking, overdosed one too many times, or have significant medical problems due to the SUD.
-
Initiating medication is easy. Medications for substance use disorders that can be initiated safely in the ED are:
-
Opioid use disorder: Buprenorphine and Methadone
-
Alcohol use disorder: Naltrexone and Gabapentin
-
Tobacco use disorder: Nicotine-replacement therap
-
-
It's not often we can actually change the trajectory of a patient's life. Initiating MAT can do just that.